- 65 Mario Capecchi Drive, Salt Lake City, Utah,84132
- 175N 400W, #C10, Orem, Utah,84057
- 2255N 1700W, Layton, Utah,84041
- 617 E. Riverside Drive, St. George, Utah,84790
- 552 N. Dixie Drive, St. George, Utah,84770
- Harley Street, London, ,W1G8
- 1025 E. 3300 S., Suite B, Salt Lake City, Utah,84106

Orbital Fracture

-
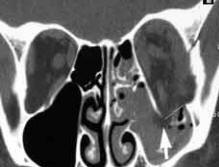
A wide range of ocular trauma can occur concomitant with orbital fractures. The ocular Sequelae of mid-facial fractures are usually considered to be edema and ecchymosis of the soft tissues, subconjunctival hemorrhage, diplopia, iritis, retinal edema, Ptosis, enophthalmos, ocular muscle paresis, mechanical restriction of ocular movement and nasolacrimal disturbances. More severe injuries such as optic nerve trauma and retinal detachments have also been reported. Noted rates of intraocular injury range from 1% to nearly 70%
-
The relationship, if any, between the purity of orbital fractures and their secondary ocular problems has not been elucidated to date.
- Intraocular injuries occur in a wide pattern when orbital bones are fractured. While several studies have reminded the community of the importance of the ophthalmic examination in patients who sustain orbital fractures, to date, there have been only a handful of studies which focus on the incidence of intraocular injuries in patients with fracturesOcular Injury
-
Of these, there is no agreement as to the incidence of injury. It is likely that the specialty of the physician conducting the research might account for the inconsistencies. In contrast, since our hospital protocol requires that all orbital fractures receive an ophthalmic examination, we believe that our results are unbiased; the true incidence of intraocular injury is approximately 17%.
Diplopia field: limit on up or downgaze: r/o IR entrapment vs hemorrhage/edema alone: CTEvaluation - Full Ophthalmic Exam Plus
-
Hertel
-
hypo-ophthalmos (globe ptosis)
-
orbit/lid emphysema 2nd to sinus wall fracture
-
IOP straight and upgaze (might inc w/IR entrapment)
-
infraorbital anesthesia in floor fracture
-
forced generation, forced duction
-
lid measurements (PF and MRD1)
 |
 |
 |
 |
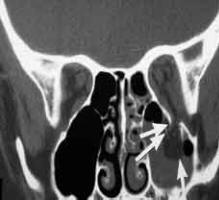
The rates of injury were also compared between pure orbital floor fractures (only floor) and impure (floor and rim). Of patients who sustained a pure orbital floor fracture, intraocular injuries occurred in 5.6%, compared with only 2% that sustained an impure fracture. Intraocular injuries are more common in patients who sustained PURE orbital fractures than in patients with rim involvement (IMPURE) (p=0.05). This difference suggests that the mechanism of injury might not be the same in each; it might not simply be solely direct force transmitted to the rim as the buckling theory suggests.Intraocular Injuries
-
Recall that the "retropulsion" theory refers to a fracture of the orbital floor caused by sudden increase in intraorbital pressure (BLOW-OUT) which occurs when an object with sufficient force hits the aperture of the orbit and forces the soft orbital contents posteriorly. Such trauma is created by objects larger than the horizontal diameter of the orbit, such as from a fist or a ball. On the other hand, the "buckling theory" proposes that the force transmitted through the rigid orbital rim directly to the thin floor , causes the floor to fracture, usually leaving the rim intact.
-
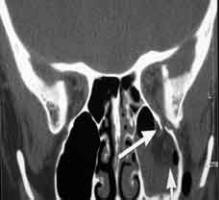
If we accept that impure fractures are the result of direct trauma to the orbital rim and resultant buckling of the floor, then we would expect similar rates of intraocular injury between pure and impure orbital fractures. This would be the case IF the buckling theory is the correct theory for pure fractures, since both are created by the same direct force to the rim.
-
However, we find that the incidence of injury is significantly higher in the pure fracture group suggesting that a different mechanism is at play. It is more reasonable to envision that the acute rise in orbital pressure would lead not only to the floor fracturing, but also to a greater incidence of intraocular injury as the globe retropulses. One could argue, however, that in the case of the impure fracture, the rate of injury is lower because the force is blunted by the rim. Nevertheless, we believe that these data suggest that the retropulsion theory might be the more likely explanation for orbital fractures; one theory (retropulsion) can explain variations of ocular findings in both pure and impure fractures
.jpg "Buckling Theory of Orbital Floor Fracture")
.jpg "Globe-to-Wall Theory of Orbital Floor Fracture")
.jpg "Retropulsion Theory of Orbital Floor Fracture")
Buckling:
- It states that the orbital rim buckles and transmits forces to the orbital walls, resulting in an orbital floor fracture.
Retropulsion:
-
The "retropulsion" theory, advanced by Smith and Regan, refers to a fracture of the orbital floor caused by sudden increase in intra-orbital pressure; a fracture might result from the hydraulic forces generated in the closed orbital cavity.
-
Blows from a fist, for instance, or objects larger than the horizontal diameter of the orbit, are the most frequent cause of this type of fracture
Globe to Wall:
Consequences of trauma
Double Vision
-
Results from an inability of both eyes to move equally
-
The "buckling" theory maintains that an anterior force is transmitted back into the orbit.
-
See pre-operative and post-operative photos below illustrating down gaze limitation of the right eye.
Illustrations of relevant orbital anatomy





Surgery Indications
|
|
|
|
|
|
|
|


Medial Orbital Fracture
-
if indirect (blowout) extension of floor fracture, no surgery needed unless medial rectus (MR) entrapped
-
lid/orbit emphysema common
-
direct naso-orbital fracture more serious, depressed nasal bridge; compl inlc cerebral/ocular damage, ant ethmoid art. damage with severe epistaxis, CSF rhinorrhea, traumatic telecanthus, needs miniplate stabilization
Zygomatic Fracture
-
tripod fracture often has 4 zygoma breaks at lateral & inferior orb rim, zygoma arch, lateral wall of maxillary sinus
-
can involve orb floor
-
if displaced, can have cosmetic deformity, trismus (2o to impingement on coronoid process of mandible)
Orbital Apex Fracture
-
often w/traumatic optic neuropathy (needs spinal cord dose IV steroids, maybe decompression w/in 5 days, see neuro-op), other fractures
-
look for CSF rhinorrhea, cartoid-cavernous (CC) fistula
Orbital Roof Fracture
-
infrequent
-
might have intracranial lesions, CSF rhinorrhea, pneumocephalus
-
neurosurgery consult
Orbital Emphysema
-
if severe can cause CRAO, etc if loculated ball valve type wound
-
usually smaller medial wall injuries
-
air usually located in area of wound
-
if decreased Vision, high dose steroids
-
air decompression:
-
CT for localization
-
retrobulbar needle into air pocket
-
fill syringe with saline, take out plunger, watch for bubbles to appear
-
look on CT for intracranial air: needs neurosurgery consult
Treatment
-
most fractures do not require surgery
early surgery for marked muscle restriction confirmed on CT, forced duction
should observe 1-2 weeks, oral steroids (prednisone 1 mg/kg/day with taper) to decrease swelling and fibrosis
antibiotics (Keflex) and nasal decongestants (Afrin), tell patient not to blow nose to decrease orbital emphysema


")



